

AIZAh KASHIF
she/her | age 15 | Ottawa, ON
Edited by Sara Peitropaulo
The effectiveness of monoclonal antibody therapy in rheumatoid arthritis was determined by analyzing three clinical trials performed by researchers from multiple regions in the world. Each trial involved patients with severe rheumatoid arthritis receiving the CD4 antigen for a set period (7 days, 18-30 months, and 4 weeks for each trial respectively) while suspending the administration of all previous medications. The combined results of the investigations display that monoclonal antibody treatment against the CD4 antigen proves to lessen the symptoms of rheumatoid arthritis in patients for the duration of the trials, while the long-term effectiveness of the drug remains unknown. Despite the open-ended results of the assessments, the adaptability and precision of monoclonal antibody treatment offer a fascinating prospect for the development of new immunotherapies and molecular drugs in the future.
INTRODUCTION
Background: RA
One of the three most common types of arthritis, rheumatoid arthritis (RA), is a chronic inflammatory disorder that can arise at any age but tends to occur between ages 30 and 50 (Marieb & Hoehn, 2018, p. 275). Affecting almost three times as many men as women, around 1% of all people globally are impacted by this disorder. In various cases, the inflammation associated with this disease can proceed to damage a wide variety of body systems beyond just the joints, including the skin, eyes, lungs, heart, and blood vessels. Over time as this continues, joints can shift out of place and cause deformities. Some of its manifestations involve osteoporosis, anemia, muscle fragility, and cardiovascular complications.
Like any other type of arthritis, RA is an autoimmune disease — a disorder in which the body attacks its own tissues (Marieb & Hoehn, 2018, p. 275). While bacteria and viruses have been suspected as the initial trigger for this reaction, the exact cause for this behaviour remains unknown. One postulation is that molecules contained in these microorganisms are similar to some innately present in the joints. This could include glycosaminoglycans (complex carbohydrates found in cartilage), joint fluid, and other connective tissues.
RA begins to manifest when the synovial membrane of the affected joints (synovitis) becomes inflamed, causing inflammatory cells from the blood, such as lymphocytes (a type of white blood cell contains T cells and B cells) and macrophages (larger white blood cells that specialize in processing cellular debris) to travel into the joint cavity and release a torrent of inflammatory chemicals with the capability to destruct body tissues when released in large amounts. This causes synovial fluid (Figure 1) to build up, resulting in joint inflammation. Although the disease can still cause major physical disabilities in extreme conditions, many drugs and treatments have been developed to attempt to treat the impairment of joint movement and severe pain in RA. (Marieb & Hoehn, 2018, p. 275).

Figure 1: Cross-section diagram of a synovial joint (Marieb & Hoehn, 2018).
There are several methods to treat RA, such as using steroidal and nonsteroidal anti-inflammatory drugs, immune suppressants (such as methotrexate), and other biological agents to block the activity of inflammatory chemicals. However, many of the treatment goals are to simply alleviate the patients’ symptoms. The ground-breaking discovery of monoclonal antibodies (mAbs) and their use in immunotherapy poses a way for RA treatment to go further than simply reducing the symptoms and to, instead, find a procedure to completely obstruct the ongoing destruction of the joints.
Monoclonal antibodies are artificially engineered proteins for a single antigenic determinant to replicate antibodies that are normally released by the immune system by researchers in a lab. They are part of a subclass of therapeutic medications known as biologics, which are used to treat autoimmune (AI) disorders including rheumatoid arthritis (RA), as well as certain cancers, viral infections, gastrointestinal ailments, and more in the field of immunotherapy (Eustice, 2022).

Figure 2: Diagram of mAbs attaching to specific proteins and alerting the immune system’s defence (LFCT, 2017).
Roles and Interactions of Antigens and Antibodies
When effector B cells (also called plasma cells) produce a protein known as an antigen (foreign material) in healthy immune systems, white blood cells release antibodies in response to bind specifically with that antigen (Marieb & Hoehn, 2018, p. 798). This is to flag other components of the immune system to fight off any viruses or threats that the antigens could pose to the body by either neutralizing them or destroying them (Figure 2). The role of monoclonal antibodies is to circulate in the body and bind to a specific antigen to destroy or neutralize it in a similar method. Researchers need to first pinpoint the exact antigen that is causing the infection in the body before developing an antibody to treat it successfully. Once the antigen has been identified, scientists can create replications or clones of the antibodies (Marieb & Hoehn, 2018, p. 798). The primary advantage of mAb treatment is that it can target antigens at the source, without damaging normal healthy cells, instead of working to lessen the progression and symptoms of the disease. This form of treatment also proves to lower the rates of death and hospitalizations in patients who are non-hospitalized with a risk of extreme disease progression (Brobst & Borger, 2022). In contrast, some negative symptoms may be irritation or infections at the location of the infusion or subcutaneous injection (Cleveland Clinic, 2021), or anaphylaxis (Eustice, 2022).
Monoclonal antibody treatment falls into three categories: anti-inflammatory, anti-cancer, and anti-viral. This investigation further expands on mAbs in anti-inflammatory diseases through their use in RA.
CD4 Antigens
One of the most significant participants in autoimmune diseases is the CD4+ T cell which can shape the nature of immune responses through their unique functions (Dittel, 2008). Researchers have determined that CD4+ T cells have a large influence in engendering various elements of autoimmune inflammation, especially in rheumatoid arthritis (Skapenko et al., 2005).
Anti-CD4 mAb: As a co-receptor for HIV, this antibody plays a large role in the identification of MHC class II molecules. In viral and autoimmune diseases of the central nervous system, it serves as a crucial intermediary of direct neuronal impairment. It must be administered by the patient’s healthcare provider’s clinic or office through subcutaneous injection or intravenous infusion (IV). Anti-CD4 mAbs are utilized as treatment to combat the symptoms of RA in all the investigations analyzed in this paper.
RESEARCH QUESTION
This study aims to investigate the extent of the effectiveness and usefulness of monoclonal antibodies in treating rheumatoid arthritis. Since rheumatoid arthritis is an autoimmune disorder, investigating immunotherapeutics is a promising avenue for future treatments. Within this field, monoclonal antibodies have begun to rise as a new therapeutic drug available for patients, making it important that we grasp its efficacy shown through observations recorded in real human trials.
MATERIALS & METHODS
Monoclonal Antibodies
In RA, monoclonal antibodies treat the disease by attacking specific proteins, such as cytokines, which have been recognized for being part of the destructive inflammation process that takes place in several arthritic and autoimmune disorders. Secreted by T cells to help amplify and regulate a variety of adaptive and innate immune responses, cytokines act as mediators that influence cell development, differentiation, and responses in the immune system (Marieb & Hoehn, 2018, p. 805). However, over time monoclonal antibodies have been developed to combat these proteins.
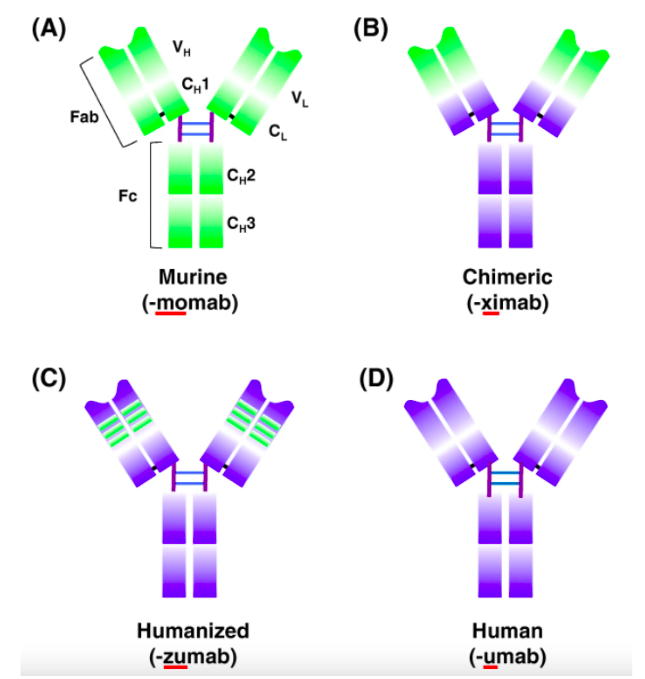
Figure 4: Diagrams of the four types of monoclonal antibodies (Lu et al., 2021).
The newest generation of monoclonal antibodies is referred to as fully humanized monoclonal antibodies. There are two routes to create these humanized monoclonal antibodies. The first method, which is used to make panitumumab, is the result of mice being genetically engineered to carry human antibody genes instead of mouse antibody genes. In most human diseases, human monoclonal antibodies are used since they have proven to be the most successful due to the wider range of antigens they can target (Harris, 1998). However, due to the established reputation of the hybridoma technology, which is a method of creating large amounts of cloned monoclonal antibodies, the development of the less costly and high affinity murine monoclonal antibodies (Figure 4) continues (Funfrock, 2019).
The second method, which is used to make adalimumab, identifies ideal CDRs using phage display by placing a genetic library of CDRs into bacteriophages. Then, the screening of the CDRs exhibiting the strongest antigen binding is allowed, due to the CDR expression from the phages. The most effective CDRs are then grafted onto a scaffold made of a human antibody (Scientific Writing Team, 2018).
Research Methods
To assess the efficacy and quality of monoclonal antibody treatment in rheumatoid arthritis, this paper focuses specifically on the use of anti-CD4 monoclonal antibodies for treatment in three separate clinical trials. To determine what trials to analyze in the research, results from multiple regions including Erlangen, Birmingham, Leiden, and London were assessed in the form of scholarly articles. Additionally, the trials analyzed in this paper were randomly selected to attempt to decrease the extent of bias from obstructing results. The goal of these factors was to expand on monoclonal antibody use in clinical environments outside of a North American viewpoint. Due to this fact, it is important to note that all results reflect a heavily Western perspective.
The first clinical trial was performed by Gerd Horneff MD, Gerd R. Burmester MD, Frank Emmrich MD, and Joachim R. Kalden in 1991. In 10 patients with severe intractable rheumatoid arthritis, the effects of therapy with a monoclonal antibody against the CD4 antigen found on T helper cells were examined. To execute the study, the monoclonal antibody anti-CD4 16H5 was infused at a dosage of 0.3 mg/kg of body weight on 7 consecutive days in an open trial.
The second clinical trial was performed by Larry W. Moreland MD, Parks W. Pratt MD, Ralph P. Bucy MD, Ph.D., Bettie S. Jackson RN, Janie W. Feldman MT (ASCP), and William J. Koopman MD in 1994 at the University of Alabama at Birmingham. Their study used a chimeric anti-CD4 monoclonal antibody (cM-T412) to assess the amount of CDR+ T cells in patients with rheumatoid arthritis after 18 and 30 months post-treatment. 25 patients with rheumatoid arthritis received a monoclonal antibody dosage; among them, 23 were available for follow-up at 18 and 30 months. To measure the levels of CD4+ T cells circulating in the body, flow cytometry was used.
The third study was executed in 1995 by researchers from the University Hospital Leiden and the United Medical and Dental Schools of Guy's and St. Thomas' Hospitals, including Paul P. Tak MD, Peter A. Van Der Lubbe MD, Alberto Cauli MD, Mohamed R. Daha MD, Tom J. M. Smeets, Philip M. Kluin MD Ph.D., A. Edo Meinders MD Ph.D., Ghada Yanni MD MRCPI, Gabriel S. Panayi ScD MD FRCP, and Ferdinand C. Breedveld MD Ph.D. Their goal was to evaluate their anti-CD4 clinical trial by considering the impact of chimeric anti-CD4 monoclonal antibody therapy on synovial inflammation. The observations were collected before anti-CD4 MAb (cM-T412) therapy and 4 weeks after, by assessing the immunohistologic features of synovial biopsy specimens in patients 7 with rheumatoid arthritis. For 5 consecutive days, patients intravenously either received daily dosages of placebo (n = 1) or 10 mg (n = 4), 25 mg (n = 2), or 50 mg (n = 1) of cM-T412.
RESULTS
Below, the effectiveness and success of these trials will be assessed. The extent to which monoclonal antibodies can treat rheumatoid arthritis will be identified through the quantitative results of each finding.

Figure 5: Diagram of chronic spontaneous urticaria symptoms in patient trials (Orzan et. al, 2022).
The results of the first trial proved that anti-CD4 monoclonal antibodies are successfully able to decrease the amount of CD4+ T cells in the body. An hour after the first infusion of the drug, observations of the kinetics showed that CD4+ T cells reduced to as low as 25 cells/μl. Then, 24 hours after the infusion, the number of recovered CD4+ T cells in that time remained lower than the original number, and 7 days after the full treatment cycle had been complete, there was still a report of a considerable decline (mean ± SD 51 ± 28%; P < 0.02). Among the 10 patients, 2 started receiving symptoms of urticaria (itchy red rash or welts caused by an allergic reaction), which led to the withdrawal of 1 from the trial (Figure 5). Another 2 patients experienced symptoms of chills with fever, representative of a lymphokine release syndrome. Between the 9 patients who completed the full 7-day trial, there was a clinical decline in the Ritchie index and number of swollen joints, as well as a particular reduction in lymphocyte reactivity in 5 patients, displayed by transformation assays. This differed from the unanticipated peak in the T cell response to mitogens and common antigens demonstrated in the remaining 4. However, this data is only accountable for the first 6 months of observation post-infusion, leaving it unclear whether this form of treatment can induce remission in the long term.
The second trial proved that at 18 and 30 months after treatment, monoclonal antibodies targeting the CD4 antigen resulted in a lower-than-normal level of circulating CD4+ T cells in the 23 patients. It was also recorded that patients who received a higher dose of the therapeutic drug (300 and 700 mg), experienced a greater level of CD4+ T cell alleviation. Overall, both groups experienced protracted suppression of circulating CD4+ T cells, however, those receiving greater doses endured a greater level of that suppression. This trial establishes that among the 23 patients in this population, the ability for CD4+ T cells to regenerate is limited, as suggested by the long-term decrease in circulating CD4+ T cells. The only significant adverse effect of this trial was the death of one patient, who was also receiving methotrexate and prednisone, 18 months after acquiring 100 mg of cM-T412.
The overall results of the third clinical trial reported a significant drop in the amount of CD4+ T cells circulating in the body. Lower mean scores for expression of adhesion molecules, as well as the declined level of synovial inflammatory infiltration among the 7 patients 4 weeks after receiving cM-T412, represent this. With either 25 mg or 50 mg cM-T412, the scores for infiltration with CD4+ and other inflammatory cells also displayed a reduction post-treatment. However, in the synovial tissue, cytokines such as TNFa and interleukin-1β could still be noticed.
DISCUSSION
The results of the three trials all assemble to support the fact that monoclonal antibodies against the CD4 antigen can be used as a viable form of therapy for rheumatoid arthritis in the time frames of each respective trial. Although this concluding assessment may seem like a significant asset for pharmaceutical companies developing this drug, or medical research in general, it leaves the efficacy of the drug in the long-term unknown.
Ultimately, it is the RA patient who will be influenced greatest by the implications of monoclonal antibody treatment beyond what was recorded in the studies. Because of this fact, in future steps, the patient's perspective during treatment should be placed at a higher value, alongside the objective methods of collecting success in monoclonal antibody therapy. For example, the possible outcomes of failed monoclonal antibody therapy for rheumatoid arthritis in the long term could be the possibility of RA symptoms returning in patients who have experienced treatment, and subsequent remission of their symptoms for a certain time frame. During treatment, patients experience months of treatment cycles by staying completely committed to a new form of therapy than whichever previous drugs they were prescribed. As described formerly, it is also common for these patients to experience adverse symptoms of treatment, which can even be life-threatening. Their experience and level of comfort during treatment will play a significant role in the success of monoclonal antibodies in clinical use. This is why patient experience should maintain a greater impact in evaluating the drug’s success.
Aside from the health of the patient, the other major reason why the failure of long-term remission is harmful is that monoclonal antibody treatment is significantly expensive (Liu, 2014). The costs for monoclonal antibody therapy are not affordable for all patients with RA, so for those patients to struggle to pay for the treatment with the chance of proper results only in the short-term limits the demand. For monoclonal antibodies to become more commercially viable therapeutic drugs in the future, the costs of administration must arrive at a level that is reasonable for patients, and a need for more significant clinical effectiveness and side effects still needs to be handled.
CONCLUSION
Monoclonal antibody treatment poses an appealing option for the evolution of new molecular drugs and therapeutic agents with the specificity and adaptability they offer in treating numerous common diseases. In rheumatoid arthritis, it can be seen through multiple studies that monoclonal antibody therapy can produce positive results, portraying that inevitably therapeutic antibodies will continue to play a significant role in drug development for years to come. This is true regardless of the specific route that leads to the creation of the next generation of monoclonal antibody therapeutics. Pharmaceutical corporations are still very interested in developing monoclonal antibodies despite their limitations for clinical and diagnostic application, and this will undoubtedly determine the future of clinical and financial management, as well as the therapy of common chronic autoimmune diseases to come.
REFERENCES
American Cancer Society. (2019, December 27). Monoclonal Antibodies and Their Side Effects. American Cancer Society. https://www.cancer.org/treatment/treatments-and-side-effects/treatment-types/immunotherapy/monoclonal-antibodies.html.
Arthritis Foundation. (2021, October 15). Rheumatoid Arthritis: Causes, Symptoms, Treatments and More. Arthritis Foundation. https://www.arthritis.org/diseases/rheumatoid-arthritis.
Brobst, B., Borger, J. (2022, April 28). Benefits And Risks Of Administering Monoclonal Antibody Therapy For Coronavirus (COVID-19). National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/NBK574507/#:~:text=Monoclonal%20antibody%20therapy%20reduces%20deaths,administration%20and%20transfusion%2Drelated%20reactions.
Carter, D. (2021, November 10). (2021, November 10). T cells, B cells and the immune system. The University of Texas MD Anderson Cancer Center. https://www.mdanderson.org/cancerwise/t-cells--b-cells-and-the-immune-system.h00-159465579.html#:~:text=T%20cells%20can%20wipe%20out,of%20protein%20called%20an%20antibody.
Choy, E. H., Kingsley, G. H., Panayi, G. S. (1998, May 1). Monoclonal antibody therapy in rheumatoid arthritis. Oxford Academic Rheumatology. https://academic.oup.com/rheumatology/article/37/5/484/1783081.
Cleveland Clinic. (2021, November 16). Monoclonal Antibodies. Cleveland Clinic. https://my.clevelandclinic.org/health/treatments/22246-monoclonal-antibodies.
Covid-19 Real-Time Learning Network. (2022, March 1). Anti-SARS-CoV-2 Monoclonal Antibodies. Covid-19 Real-Time Learning Network. https://www.idsociety.org/covid-19-real-time-learning-network/therapeutics-and-interventions/monoclonal-antibodies/.
Dittel, B. N. (2008, January 18). CD4 T Cells: Balancing the Coming and Going of Autoimmune-Mediated Inflammation in the CNS. National Library of Medicine. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2376206/#:~:text=In%20a%20T%20cell%2Dmediated,central%20nervous%20system%20(CNS).
Eustice, C. (2022, July 1). Monoclonal Antibodies for Arthritis and Other Diseases. Verywell Health. https://www.verywellhealth.com/what-is-a-monoclonal-antibody-189490.
Funfrock, P. (2019, October 7). Are murine monoclonal antibodies still relevant for modern medicine? ProteoBlog. https://www.proteogenix.science/scientific-corner/antibody-production/murine-monoclonal-antibodies-and-their-use-in-modern-medicine/.
Grassi, W., De Angelis, R., Lamanna, G., Cervini, C. (1998, December 10). The clinical features of rheumatoid arthritis. Science Direct. https://www.sciencedirect.com/science/article/abs/pii/S0720048X98000382.
Harris, W. J. (1998). Humanized Antibodies. Encyclopedia of Immunology (Second Edition). https://www.sciencedirect.com/topics/neuroscience/humanized-antibody.
Horneff, G., Burmester, G. R., Emmrich, F., Kalden, J. R. (1991, February). Treatment of rheumatoid arthritis with an anti-CD4 monoclonal antibody. Wiley Online Library. https://onlinelibrary.wiley.com/doi/abs/10.1002/art.1780340202.
Liu, J. K. H. (2014, September 11). The history of monoclonal antibody development – Progress, remaining challenges and future innovations. National Library of Medicine. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4284445/#:~:text=From%20the%20time%20the%20first,range%20of%20diseases%20and%20conditions.
LFCT. (2017, June 14). Monoclonal Antibody Therapy in Cancer Treatment. Little Fighters Cancer Trust. https://littlefighterscancertrust.wordpress.com/2017/06/14/monoclonal-antibody-therapy-in-cancer-treatment/.
Lu, R.- M., Hwang, Y.- C., Liu, I.- J., Lee, C.- C., Tsai, H.- Z., Li, H.- J., Wu, H.- C. (2020, January 2). Development of therapeutic antibodies for the treatment of diseases - Journal of Biomedical Science. BioMed Central. https://jbiomedsci.biomedcentral.com/articles/10.1186/s12929-019-0592-z.
Mareib, E. N., Hoehn, K. (2018, January 5). Human Anatomy and Physiology (Eleventh Edition). Pearson. file:///Users/aizah/Downloads/Elaine%20N.%20Marieb,%20Katja%20Hoehn%20-%20Human%20Anatomy%20and%20Physiology.pdf.
Mayo Clinic. (2021, May 18). Rheumatoid arthritis. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/rheumatoid-arthritis/diagnosis-treatment/drc-20353653.
Mayo Clinic. (2021, November 9). Monoclonal antibody drugs for cancer: How they work. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/cancer/in-depth/monoclonal-antibody/art-20047808.
Moreland, L. W., Pratt, P. W., Bucy, R. P., Jackson, B. S., Feldman, J. W., Koopman, W. J. (1994, June). Treatment of refractory rheumatoid arthritis with a chimeric ANTI-CD4 monoclonal antibody. Wiley Online Library. https://onlinelibrary.wiley.com/doi/abs/10.1002/art.1780370610.
National Cancer Institute. (n.d.) interleukin. National Cancer Institute. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/interleukin.
National Cancer Institute. (n.d.). monoclonal antibody. National Cancer Institute. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/monoclonal-antibody.
Orzan, O. A., Popa, L. G., Mihai, M. M., Cojocaru, A., Giurcăneanu, C., & Dorobanțu, A. M. (2022). Current and Future Approaches in Management of Chronic Spontaneous Urticaria Using Anti-IgE Antibodies. Medicina. https://doi.org/10.3390/medicina58060816.
Pope, A. (2021, August 23). Five questions about monoclonal antibodies. The University of Alabama at Birmingham. https://www.uab.edu/news/health/item/12241-five-questions-about-monoclonal-antibodies#:~:text=%E2%80%9CMonoclonal%20antibodies%20are%20supplemental%20antibodies,first%2010%20days%20of%20symptoms.%E2%80%9D.
Rankin, E. C. C., Isenberg, D. A. (2012, November 18). Monoclonal Antibody Therapy in Rheumatoid Arthritis. SpringerLink. https://link.springer.com/article/10.1007/BF03259511.
Scientific Writing Team. (2018, January 23). Monoclonal Antibodies: Past, Present and Future. Nuventra. https://www.nuventra.com/resources/blog/monoclonal-antibodies-past-present-and-future/.
Skapenko, A., Leipe, J., Lipsky, P. E., Schulze-Koops, H. (2005, March 16). The role of the T cell in autoimmune inflammation. National Library of Medicine. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2833981/.
Tak, P. P., Van Der Lubbe, P. A., Cauli, A., Daha, M. R., Smeets, T. J. M., Kluin, P. M., Meinders, A. E., Yanni, G., Panayi, G. S., Breedveld, F. C. (1995, October). Reduction of synovial inflammation after anti-cd4 monoclonal antibody treatment in early rheumatoid arthritis. Wiley Online Library. https://onlinelibrary.wiley.com/doi/abs/10.1002/art.1780381012.
Thermo Fisher Scientific. (n.d.). CD4 Antibodies. Thermo Fisher Scientific. https://www.thermofisher.com/antibody/primary/target/cd4#.
Van Der Lubbe, P. A., Dijkmans, D. A. C., Markusse, H. M., Nässander, U., Breedveld, F. C. (1995, August). A randomized, double-blind, placebo-controlled study of cd4 monoclonal antibody therapy in early rheumatoid arthritis. Wiley Online Library. https://onlinelibrary.wiley.com/doi/abs/10.1002/art.1780380812.
Wendling, D., Racadot, E., Wijdenes, J., Sibilia, J., Flipo, R. M., Cantagrel, A., Miossec, P., Eschard, J. P., Macro, M., Bertin, P., Lioté, F., Debiais, F., Juvin, R., Le Goff, P., Masson, C. (1998, August 1). A randomized, double blind, placebo controlled multicenter trial of murine anti-CD4 monoclonal antibody therapy in rheumatoid arthritis. Europe PMC. https://europepmc.org/article/med/9712083.
ABOUT THE AUTHOR

Aizah Kashif
Aizah Kashif is a Grade 11 student studying at Colonel By Secondary School. Intrigued by the complexities of psychology and biotechnologies developed to treat and diagnose medical disorders, she looks forward to delving deeper in the biomedical field. As an enthusiastic Community Engagement Coordinator for Stem Fellowship, she is also interested in reading books, showcasing her visual art skills, and learning new skills. Aizah looks forward to more opportunities to share her work in the future.